

Working with Workflow: Long-term care’s EMR Technology
When long-term care (LTC) first started to move from paper to electronic information systems, we took our workflow check-off sheets and digitized them without thinking much about the new workflows that would be required to take advantage of the new application. This usually happened because we were in a hurry to get the new application online.
But upgrading your technology is much more than reproducing old workflows on a prettier screen with fewer clicks. It’s advisable to examine workflow long before an upgrade or new installation and introduce improvements in clinical care, productivity and efficiency.
Most of today’s leading information technology (IT) vendors do their best to help providers look at clinical and financial workflows, but the pressure and costs of implementation sometimes result in inadequate analysis of today’s required workflows. The study of future workflows based on national programs usually does not happen at all. In previous blogs I’ve pointed out the value of having a dynamic HIT Strategic Plan. If you have done this, you’ve started to look at future workflows. But, your first priority probably is choosing a vendor and application. Your second priority will be the training of the users. Being realistic, most providers focus on today’s issues rather than the future workflows and how they will fit into your strategic HIT plan, especially since all the changes in care and payment models make the future a challenge to predict.
I think it’s important to try to visualize what your skilled nursing facility or home care agency might look like in 2015. A year when there is a national HIT infrastructure to support person-centric, longitudinal electronic medical record (EMR) as well as interconnectivity and interoperability through transitions of care. A projected healthcare future where long-term and post-acute care providers are not silos of care, but are activily engaged throughout the spectrum of care. I can only imagine the trauma of being a project leaders for a new HIT infrastructure implementation and having to know the ultimate clinical and financial workflow in a person-centric, longitudinal care world. When you think about it, it is almost an overwhelming project.
Over the past month I have been working with a number of thought leaders from the Renaissance Technology Consultants Group, LLC in Reading, Mass. on the issue of unbundling workflow. Our goal was to develop a better, less intimidating definition of workflow. We determined that providers should think about workflow in stages over a long period of time, not just when they’re implementing a new enterprise application. We came up with a simple list of workflow stages so that people can understand the timeframes without becoming threatened by the magnitude of workflow change. Remember, changing your HIT infrastructure is an evolution and not a revolution—so take your time. Timing is also influenced by national and regulatory policy. A provider cannot move too fast, since as changes are happening all along the timeline.
The graphic below shows the unbundling of workflow into workable stages.
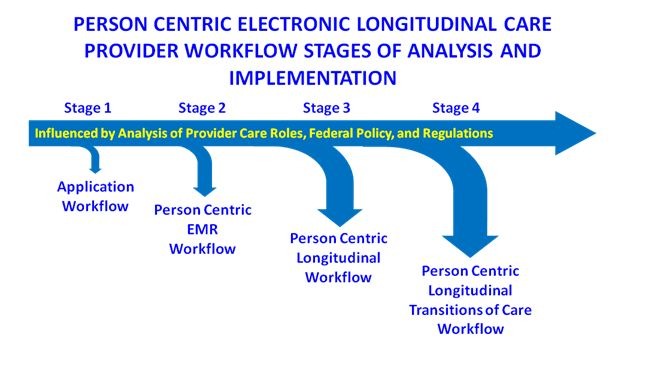
Stage 1– Workflow research and analysis is accomplished with the vendor and provider teams before starting the training and implementation of the software application. The initial workflow requirements are designed to implement the application with a minimum disruption of quality of care and the business. This launches the basic requirements of a person-centric EMR.
Stage 2– Workflow analysis is accomplished after the basic person-centric EMR workflow has been fully implemented and in use for a reasonable period of time. Additional elements of care including laboratory, radiology, therapy and pharmacy medication management complete the provider’s EMR.
Stage 3 – Workflow expands the person-centric EMR longitudinally by time and dynamic trending. Clinical alerts and eDecision (Clinical Decision Support) software are added so that person-centric care coordination teams can begin to provide proaction, prevention and wellness care plans.
Stage 4– Workflow takes the person-centric longitudinal EMR and incorporates transitional care technology to receive care record information that has been gathered by other providers upon intake, and to transmit information back to a care record upon discharge for use by the next provider or by the individual themselves.
In today’s world of the HITECH Act, healthcare information exchanges and 30-day re-hospitalizations, sometimes interconnectivity with the hospital and physician has to follow Stage 1. In this case, minimum electronic transitions of care patient information will be exchanged before the LTC provider has moved past a basic person-centric EMR. This is acceptable as long as both the hospital and LTC provider realize that this is merely the first step towards the ultimate goal of implementing all four stages of workflow.
I hope this helps to put workflow in perspective and suggests that total patient-centric longitudinal care workflow does not have to all happen at once. Providers have to evolve their workflows over time, but they also should realize that healthcare workflow needs to be is not about dynamic, personal and longitudinal care—not the static, episodic care of the past.

John Derr, RPh, currently serves as Health Information Technology Strategy consultant to Golden Living, where he previously served as CIO and CTO. He is currently on the HHS Federal Advisory Committee on Standards, a CCHIT Trustee, and serves on several other federal and state HIT advisory groups. His extensive career has included major executive positions with Squibb, Siemens, Tenet (NME) and AHCA/NCAL. With almost 50 years of experience in healthcare, Derr has also started four companies.
Related Articles









Topics: Technology & IT