

The shock of elder abuse in assisted living
If you’re an executive director of an assisted living community, you may not be aware of all of the cases of elder abuse—especially sexual incidents—occurring there.
That’s the conclusion of Marguerite “Marti” DeLiema, a doctoral candidate at the University of Southern California’s (USC's) Davis School of Gerontology. DeLiema discussed elder abuse with the more than 100 people attending the Assisted Living Federal of America (ALFA) Executive Director Leadership Institute (EDLI), held in conjunction with ALFA’s recent annual meeting. As part of her session, she polled attendees about their observations or suspicions of staff members’ physical mistreatment of residents, mismanagement of resident medication (stealing residents’ medication for themselves, giving medication intended for one resident to another resident, or withholding medication from a resident) and inappropriate sexual behavior with residents within the past year. She also reviewed the results of her informal survey later in a general session, which I attended.
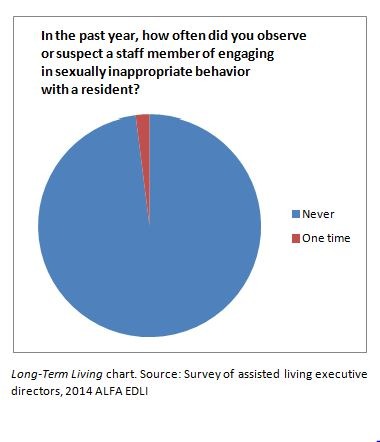 When it came to physical mistreatment of residents or mismanagement of medication, EDLI participants’ reporting of observed or suspected incidents was similar to that of assisted living nurse aides surveyed by Nicholas Castle, PhD, and Scott Beach, PhD, for a large study published in the Journal of Applied Gerontology. Concerning sexually inappropriate behavior between a staff member and a resident, however, the executive directors reported a much lower frequency of this type of abuse than did the nurse aides, DeLiema told me in an exclusive follow-up interview. All but one responding executive director said they had never observed or suspected a staff member of such behavior, she says; one reported observing or suspecting one case. By comparison, the Castle and Beach study of nurse aides, DeLiema said, had “a lot more shocking results.” For instance, three percent of the nurse aides surveyed by Castle and Beach said they knew of staff members’ “unwelcome fondling” of a resident, and seven percent said they knew of staff members who had exposed a resident’s body part as a form of abuse.
When it came to physical mistreatment of residents or mismanagement of medication, EDLI participants’ reporting of observed or suspected incidents was similar to that of assisted living nurse aides surveyed by Nicholas Castle, PhD, and Scott Beach, PhD, for a large study published in the Journal of Applied Gerontology. Concerning sexually inappropriate behavior between a staff member and a resident, however, the executive directors reported a much lower frequency of this type of abuse than did the nurse aides, DeLiema told me in an exclusive follow-up interview. All but one responding executive director said they had never observed or suspected a staff member of such behavior, she says; one reported observing or suspecting one case. By comparison, the Castle and Beach study of nurse aides, DeLiema said, had “a lot more shocking results.” For instance, three percent of the nurse aides surveyed by Castle and Beach said they knew of staff members’ “unwelcome fondling” of a resident, and seven percent said they knew of staff members who had exposed a resident’s body part as a form of abuse.
“What really surprised me was the reaction of the audience to the Castle and Beach study” results related to sexual abuse, DeLiema said of EDLI participants. “They were really shocked by how high those rates were. They were shaking their heads and putting their hands over their mouths. They were really surprised. So that speaks to the fact that they just are not aware that this is going on in their communities.”
Why does this discrepancy exist between executive directors and nurse aides? One possibility, she said, is that the aides are closer to the delivery of care and so may see more incidents of inappropriate sexual interaction.
“It’s my guess that it’s just that [the executive directors are] further removed,” DeLiema told me. “These nursing aides are literally with [residents] 24/7, and they are the ones who have to manage the more difficult behaviors and do all of the personal care work. You would hope that the executive director would hear about these things if they’re being reported, but perhaps not.”
Also, she added, perhaps some incidents of abuse are handled within the nursing department and are not communicated to the executive director. Or perhaps the EDLI survey-takers hesitated to respond honestly to the question, even though they were submitting their answers electronically and anonymously during the EDLI session.
Elder abuse takes many forms—financial, sexual, physical and emotional/psychological abuse as well as neglect. What can be done to prevent and address such abuse in long-term care settings, whether it be perpetrated by a staff member, a family member or another resident? Increased awareness—through educational programs such as the EDLI and events such as World Elder Abuse Awareness Month, observed every June, and World Elder Abuse Awareness Day, observed every year on June 15—is one solution. Others, according to DeLiema:
- Develop and maintain a good working relationship with the long-term care ombudsman in your state. “Sometimes, the cases we see, the facility can only do so much. They really need to pull someone in from the outside, and sometimes, the best option is more of a mediator than the police or adult protective services,” she said, noting that ombudsmen usually take a person-centered approach.
- Educate residents, family and staff members that reporting abuse is a good thing. “You really need buy-in from the older adults if you’re going to try to ‘protect’ them,” DeLiema said. “And the same with physicians, getting them to feel that reporting is the best option” rather than trying to address incidents directly themselves.
- Train direct care staff who work with combative residents so that they don’t react in an abusive way to behaviors that, because of a cognitive disease process, may be beyond a resident’s control. “It’s important that they have a good understanding of the disease process,” DeLiema said. Training, she added, can answer these questions: “What is cognitive impairment, how does it manifest, what kind of behaviors can they expect?”
- Establish a system to address suspected or confirmed incidents of staff mistreatment of residents to ensure that such incidents don’t recur.
The USC Davis School of Gerontology touts that it is the oldest and largest such school in the world. DeLiema also points executive directors and others to the school’s website and its Guide for Elder Abuse Response (GEAR) website and app as additional resources. The app, she noted, has some elements of particular interest to those working in California, where the school is located, but it also contains information of wide potential interest.
I Advance Senior Care is the industry-leading source for practical, in-depth, business-building, and resident care information for owners, executives, administrators, and directors of nursing at assisted living communities, skilled nursing facilities, post-acute facilities, and continuing care retirement communities. The I Advance Senior Care editorial team and industry experts provide market analysis, strategic direction, policy commentary, clinical best-practices, business management, and technology breakthroughs.
I Advance Senior Care is part of the Institute for the Advancement of Senior Care and published by Plain-English Health Care.
Related Articles








Topics: Executive Leadership , Leadership , Risk Management , Staffing