

Health information technology in LTC: Where do we stand?
In this new monthly blog, I will bring you the big picture in long-term and post-acute care (LTPAC) health information technology, and inform you on how to participate in the future—so we in long-term post-acute care can control our future, through strategic planning.
I will look at the total LTPAC picture. This includes research supplied by the Center for Aging Services Technologies and case studies documented by providers who are or have adopted a clinical technology infrastructure.
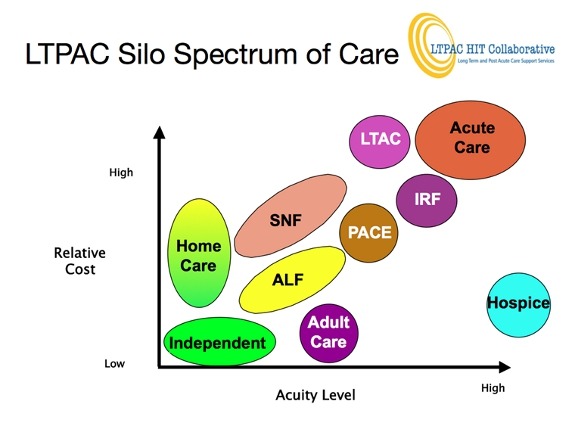
The above is a simple illustration of the providers in LTPAC, which also includes information technology, telemedicine, telehealth, imaging and other technologies that provide services to LTPAC providers. Over the years, “LTC” has become synonymous with SNFs and does not represent all of the providers. The acronym LTPAC does a much better job of representing our healthcare sector.
You will also note that the providers are silos. This is mainly due to the way the providers are being paid. A 2004 Presidential Executive Order, also supported by President Obama, stated that the U.S. Healthcare System would be interoperable and interconnected via the electronic health record (EHR). This established the Department of the Office of the National Coordinator for Health Information Technology under the secretary of Health and Human Services.
When dynamic, integrated, person-centric EHRs are available through an interconnected and interoperable HIT system, the silo walls will break down. An individual—through his or her physician—will receive care that is best for them and preferably at their chosen home. Accountable care organization and accountable care community models are intended to be person-centric and break down provider silos.
For future success to occur, those person-centric EHRs must replace a provider system that is currently static and episodic. The LTPAC provider and vendor have to take this into consideration once they begin strategic planning. The provider has to determine what role they will play in providing care to an individual throughout the spectrum of care.
Lastly, I wanted to cover the groups that are directly supporting LTPAC HIT initiatives. Some providers and vendors might think after reading all of the hospital and physician information published on HITECH incentives that we in LTPAC do not have representation. This is not true. Dr. Farzad Mostashari, the national coordinator for HIT; his staff; and members of federal advisory committees all realize the value of LTPAC providers and vendors and have set up workgroups, grants and challenges to assist their involvement in HITECH activities.
There is also an LTPAC objective in the Office of the National Coordinator strategic plan, the focal point of which is the LTPAC HIT Collaborative. This group is made up of representatives from all facets of LTPAC, and its only focus is the role of LTPAC HIT in tomorrow’s healthcare system. This will be the subject an upcoming blog.
Comments and discussion are welcome. Most all associations representing LTPAC have HIT committees and information can be found on their websites. The following are some websites that are dedicated to LTPAC HIT:
National Quality Forum LTPAC Workgroup
Center for Aging Services Technologies

John Derr, RPh, currently serves as Health Information Technology Strategy consultant to Golden Living, where he previously served as CIO and CTO. He is currently on the HHS Federal Advisory Committee on Standards, a CCHIT Trustee, and serves on several other federal and state HIT advisory groups. His extensive career has included major executive positions with Squibb, Siemens, Tenet (NME) and AHCA/NCAL. With almost 50 years of experience in healthcare, Derr has also started four companies.
Related Articles









Topics: Technology & IT